NOTE 01/22/2024: The results of the new study by the Till/Lanphear team (Hall et al., 2024) do NOT show adverse effects of fluoride, as claimed by some in the anti-fluoridation movement. The small and limited effects observed are entirely in line with observed fluoride effects in humans or animals exposed to elevated iodine levels, also documented in the decades-long use of fluoride in the treatment in iodine-induced hyperthyroidism. For example, in hyperthyroid patients, any increase in TSH and a decrease in FT4 would be seen as markers that treatment is working. In that case, such results would be seen as a benefit.
However, once again it is of utmost importance to recognize that excess iodine ingestion itself may also cause an increase in TSH and a decrease in FT4 levels, as a result of iodine-induced thyroid dysfunction, commonly observed in pregnant women consuming too much iodine. This is also observed in children exposed to excess iodine (Lee et al., 2023).
It is beyond time for the York/MIREC team to accurately and properly address this issue.
It is crucial to examine iodine/thyroid status when evaluating fluoride toxicity in pregnant women and their offspring. Both mother and fetus exhibit heightened sensitivity to even slight alterations in thyroid hormone metabolism.
Fluoride toxicity depends on the individual's iodine/thyroid status. Effect modification by iodine status was NOT evaluated.
1. Adjustment for Maternal Iodine Status
QUESTION: The authors claim that they adjusted for maternal iodine status. Is this true?
ANSWER: No, not really. Not in their primary models. Iodine was not included in the main adjustment set. The authors addressed iodine only in a sensitivity analysis, where they reran significant models with Tg, UICSG, and UIC/Cr added as covariates “to evaluate potential confounding by maternal iodine status.”
[Simply including iodine as a covariate (i.e., controlling for it in the models) does not fully address whether iodine intake confounds the effects of fluoride.]
- Including iodine as a covariate does not, by itself, resolve confounding when iodine has non-linear (U-shaped) relationships with thyroid outcomes and may modify fluoride effects. In this study, the York team treated iodine as a single linear term, without quadratic or spline modeling of iodine nonlinearity and without testing effect modification across the more-than-adequate and excess iodine range.
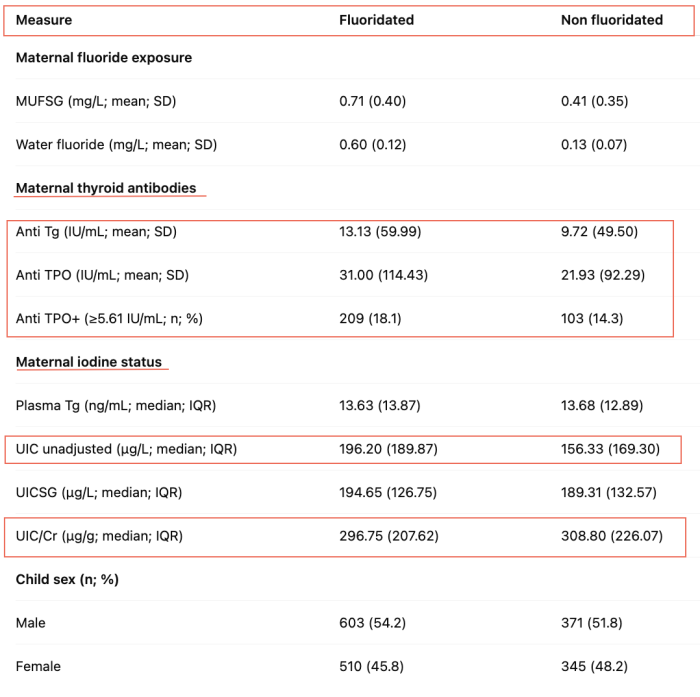
However, a core problem is that in this cohort iodine is higher in the higher-fluoride setting using the basic, unadjusted UIC measurements. (Notice that unadjusted UIC was NOT used as a co-variate!) In other words, the fluoride contrast is bundled with an iodine shift, and iodine is thyroid-relevant, of course. The very definition of a confounder applies here.
2. Iodine Status
Once again, authors here merely considered iodine "sufficiency" - or their own interpretation of such - and compared to "insufficiency".
"Insufficiency" is certainly not the problem here.
As shown below, the concerns have to do with iodine intake that is
too high, normally categorized as "more-than-adequate" or "excessive".
As discussed elsewhere, this is due to the high iodine intake from the prenatal supplements.
[88% of the pregnant women in the MIREC cohort took prenatal supplements containing approx. 220 µg of potassium iodide, resulting in an average iodine intake of 452 μg/day (Krzeczkowski et al., 2023). The WHO recommendation for daily iodine intake during pregnancy is 250 μg/day.]
"Iodine status" during pregnancy is divided into
four categories, based on urinary iodine concentrations (UIC):
- Insufficient: UIC <150 μg/L
- Adequate: UIC 150-249 μg/L
- More-than adequate: UIC 250-499 μg/L
The
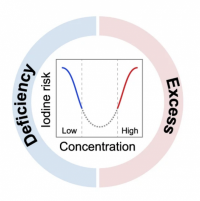
full range of iodine intake levels needs to be considered, as more-than-adequate or excessive iodine intake may impact thyroid function just like iodine deficiency.
It is well-established that the correlation between alterations in thyroid function and urinary iodine levels follows a U-shaped curve:
However, the Till/Lanphear team continually offers misleading information on this issue.
Here, the authors write:
"Controlling for maternal urinary iodine status in all models of fluoride exposure and maternal thyroid hormone levels did not change the results. Iodine is an essential nutrient for thyroid hormone synthesis and plays an important role in determining the magnitude of fluoride’s effect on the thyroid. Specifically, iodine has been found to modify the association between urinary fluoride concentration and TSH levels among pregnant women (Griebel-Thompson, 2022) and non-pregnant adults, (Malin et al., 2018) such that this association was only significant among those who were classified as iodine insufficient."
This is entirely misleading, implying that other iodine states had been investigated.
Further, neither Griebel-Thompson et al. (abstract only) nor Malin et al. (Till's team) ever considered "more-than-adequate" or "excessive" iodine intake.
In fact, that was made quite clear by Malin et al. who had
removed all participants with excessive iodine intake from their study:
"We removed these participants because excess iodine levels can cause abnormalities in TSH (Katagiri et al., 2017), including elevations, and we wanted to test the relationship between fluoride exposure and TSH as a function of iodine deficiency, not iodine excess." (Malin et al., 2018)
It should be noted that already in 2018, Malin/Till used incorrect "adequate" ranges for UIC in their model, deeming a UIC of 50-300 μg/L as "non-deficient."
[for proper UIC reference ranges in non-pregnant adults, see sidebar (below) with WHO charts]
Authors admit that they did not test for effect modification. The ignorance on "iodine sufficiency" is further displayed in the statement:
"Effect modification was not tested directly in the current study due to limited statistical power given nearly all women in the MIREC cohort were classified as iodine sufficient in a prior study (Krzeczkowski, 2023) based on our estimate of daily iodine intake."
The authors appear to misunderstand their own findings, relying on outdated Estimated Average Requirement (EAR) and Tolerable Upper Intake Level (UL) values established by the US Institute of Medicine in 2001
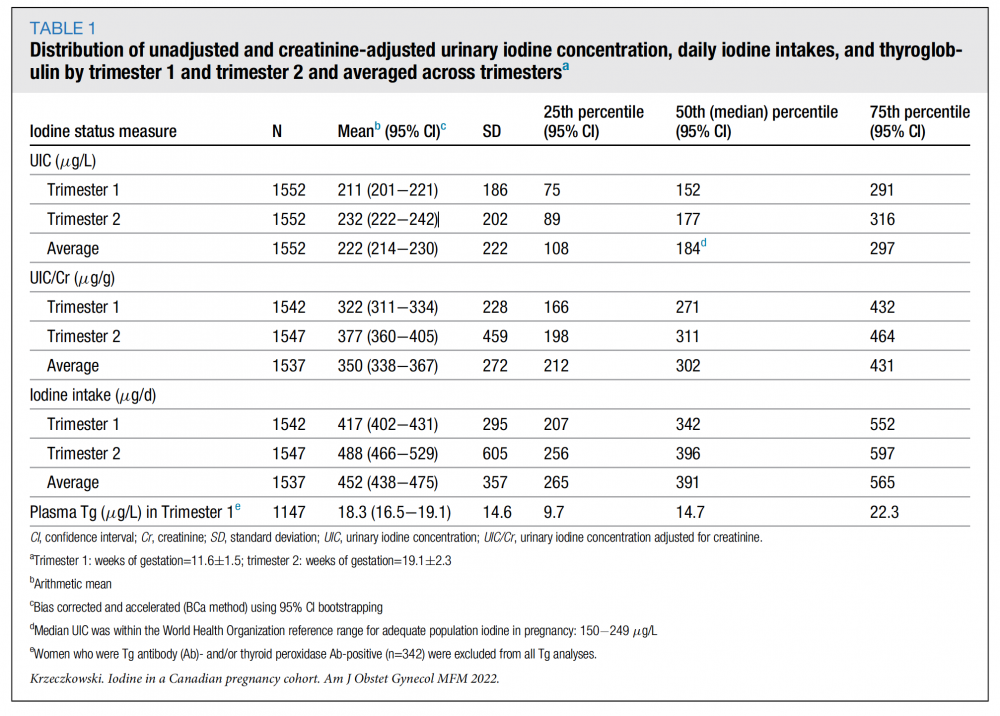
(IOM, 2001). These thresholds do not account for recent evidence highlighting the risks of elevated iodine intake, particularly during pregnancy. The Krzeczkowski (York team) paper revealed that at least 25% of the women had a UIC >250 µg/L, indicating
more-than-adequate iodine status. When using creatinine-adjusted UIC (UIC/Cr), the majority of women exceeded adequacy thresholds, despite the fact that UIC/Cr lacks standardized reference ranges and is not recommended by WHO. Furthermore, based on daily iodine intake estimates, nearly all women surpassed the WHO-recommended intake level of 250 µg/day, which is designed to prevent iodine deficiency. These findings strongly suggest that many women were at risk of iodine overexposure, a condition associated with adverse thyroid outcomes.
Here is Table 1 from Krzeczkowski et al., 2023:
 To appreciate the significance of this, it's crucial to understand that a maternal UIC exceeding 250 μg/L has been linked to:
To appreciate the significance of this, it's crucial to understand that a maternal UIC exceeding 250 μg/L has been linked to:
- Subclinical hypothyroidism (SCH) (Corcino et al., 2019; Shi et al., 2016; Wang et al., 2017; Liu et al.,; Sang et al., 2012; Yang et al., 2020)
Maternal SCH in pregnancy is associated with increased risk of adverse neonatal outcomes, including delayed intellectual and motor development, low birth weight, premature delivery, fetal distress and fetal growth restriction.
- Gestational diabetes and hypertensive disorders (Silva de Morais et al., 2020)
- Non-immune hypothyroidism (Kim et al., 2019)
- Increase in thyroid auto-immune disease (increased TPOab linked to loss of IQ in offspring) (Habimana et al., 2014; Shi et al., 2016)
- Macrosomia (LGA) (Dong et al., 2021)
- Thyroid nodules (Gao et al., 2021; 2019)
The lack of awareness on iodine needs and thyroid hormone metabolism during gestation is evident in many papers by the Till/Lanphear team. For instance, in Goodman et al. (2022), the team invented their own "adequate" range for iodine intake during pregnancy. In that study, they claimed a UIC/cr of 200-600 μg/g to be reflective of "adequate" iodine status (!).
This ignorance has evidently led to numerous modelling errors and misinterpretations, and questionable methods overall.
For example, thyroglobulin (Tg) levels were investigated as an indicator for iodine sufficiency. While Tg levels might be an adequate replacement for taking UIC measurements in
iodine-deficient populations, they have only very limited use during pregnancy, or in cases of excessive iodine ingestion. Hence, many experts have advised against using Tg levels to determine iodine status during pregnancy
(i.e. Laurberg et al., 2007; Koukkou et al., 2006).
As one can tell from Fig. 2 of the Dineva study - cited by Hall - Tg levels do
not differentiate between
adequate (UIC/cr 150-249 μg/g) and
more-than-adequate intake (UIC/cr >250 μg/g).
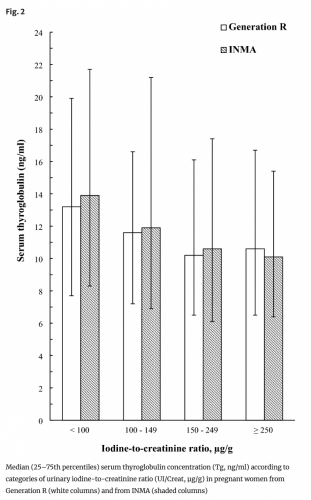
The variability and overlap of Tg levels across categories, including the more-than-adequate or excessive iodine intake groups (≥ 250 µg/g), indicate that Tg is not a reliable biomarker for distinguishing these levels of iodine intake in pregnant women. The wide error bars further suggest significant variability within each group, making it difficult to draw clear conclusions about the relationship between iodine intake and Tg levels.
SUMMARY: Contrary to their claims, the authors did
not investigate whether the relationship between fluoride exposure and thyroid hormones was modified by different states of iodine sufficiency. They did
not "adjust for maternal iodine status", and used incorrect "adequate" definitions in their models. They did not properly evaluate iodine as a confounder/modifier.
Wendy Small
PFPC Canada
DID YOU KNOW?
- High iodine intake was found to be the main cause of thyroid dysfunction among pregnant women. The prevalence of excessive iodine intake in 10,736 pregnant women in different regions of the world was 52%. (Candido et al., 2023).
- In light of recent large-scale studies showing an increase in subclinical hypothyroidism when maternal UIC is greater than 250 μg/L, calls have been made advocating that an upper level of sufficiency in pregnancy should not exceed an intake of 250 µg/day (Shi et al., 2015; Lee & Pearce, 2015).
- SIDEBAR:
Malin, Till, et al. (2018) also used a false "adequate" range in their 2018 study "Fluoride exposure and thyroid function among adults living in Canada: Effect modification by iodine status".
In that study, they classified anyone with a UIC of 50 - 300 μg/L as "not iodine-deficient".
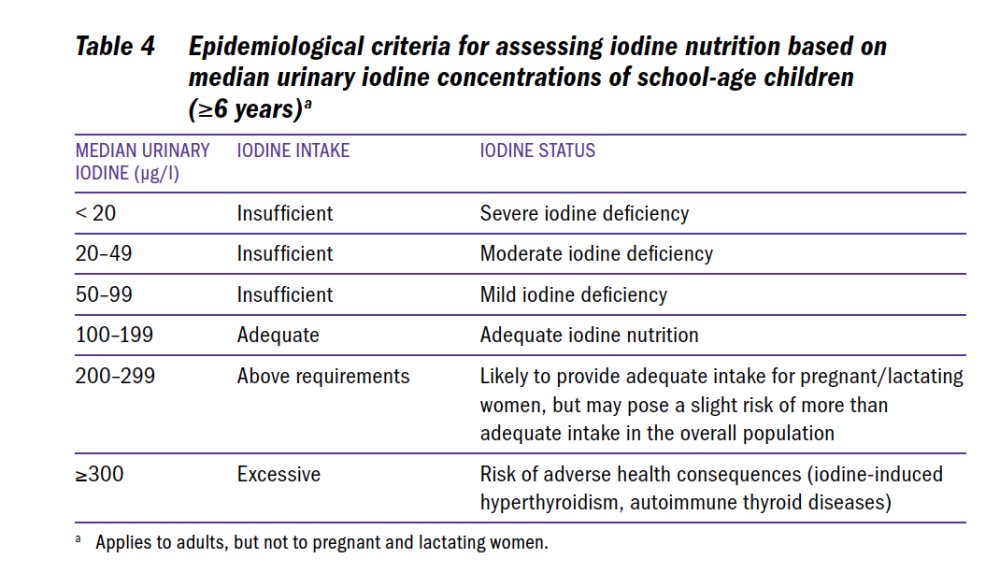
- As in Goodman (2022), the authors cite a 2004 WHO document in support of their numbers. However, that document provides the following UIC reference ranges (pg. 6) (for children >6 and adults):

It is clear that Malin, Till et al. should have used the correct established iodine status UIC reference ranges for a study on "effect modification by iodine status".
Likewise, the 2007 WHO/UNICEF Guidelines state:
 REFERENCES
REFERENCES
All references cited are listed on the "York/MIREC - FAQ References" page:
viewtopic.php?f=97&t=5022